
My rate of emission of 140 keV photons is now down to lower levels, five radioactive half lives after injection. The concentration has been reduced by biological elution and the radioactivity by decay. It was interesting to read how few suppliers there were for 99mTc. Yesterday, she only injected a few millilitres of tracer.
–

–
I have been reading up and watching videos on the interpretation of bone scans, I can probably note metastatic lesions, depletion in tracer localisation due to prothesis, fractures (old and new), areas of bone formation and depletion. It might be interesting to see what my damaged cervical spine looks like and if my “broken” ribs from rugby can be seen. Osteophytes are evident on my thoracic spine and near my Titanium pin. The Diffuse Idiopathic Skeletal hyperostosis (DISH) is probably still growing and could localise tracer. {I had a full body scan.} This, if seen, can be cross referenced with an upcoming CT scan.
There could be plenty in my scans for a nuclear medicine professional to discuss with her younger colleagues.
I meet some of the diagnostic criteria for polycythaemia (probably secondary). If it is the malignant form this may interfere with bone cycling in the marrow and could appear in the scintigraphy. There are a few suggestions in the literature to use nuclear medicine to detect this. But it is not common practice.
I guess the single-photon emission computed tomographic (SPECT) images might show something like this below. My hip arthritis is much worse than in the X-ray or CT images below. It does not look like a whole lot of extra knowledge comes from the SPECT data for the hip.
——————————————————
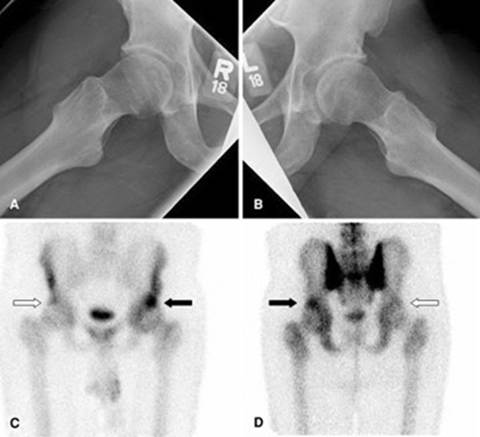
Dunn’s view of (A) right and (B) left hips of a 48-year-old male patient presenting with left hip pain only. Single-photon emission computed tomographic images shown in (C) anterior and (D) posterior coronal views display more uptake (black arrow) along the superolateral aspect of the acetabular roof on the symptomatic left hip compared with the asymptomatic right hip (white arrow).
Clin Orthop Relat Res. 2008 Dec 17;467(3):676–681
—————————————————————————–
What might however be interesting is what tips up in the rest of the body scan. The pain in my lower and mid lumbar spine has been explained in different ways by different doctors. There might be clues as to what is going on.
I guess what I do not want to see is evidence for primary bone cancer or metastatic disease. The main diagnostic differentiation of the latter is a disordered or “random” appearance of tracer localisation. Metastatic disease is incurable and often terminal.
I have joked that I could re-train as a radiographer or a nuclear medicine operator. But you know what they say about old dogs.
It is weird, I feel very up in the air, with little or no idea if/when I will get to see the data. Something which could change the direction of life is hanging ill-defined in the aether. I am in a kind of limbo.
I wonder if people who prescribe scans have ever had to wait and hang like this…
Maybe it should be a compulsory part of training…
