–
–
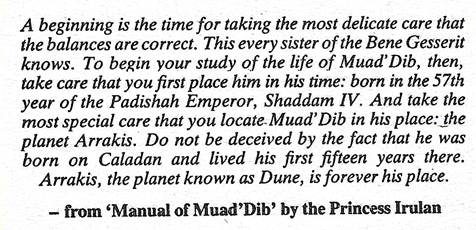
The very first sentence of the above has informed many things for me in this life. It has been a kind of a mantram for me. When I used to do team and personal development courses I found that detailed and impeccable attention to the start impacted outcome. When the balance was right things flowed well. On the occasions that someone messed with this preparation the course “went wrong”. A simple thing unbalanced at the start unleashed a chaos. People failed to appreciate this…The idea was to start “tight” and then allow things to unfold and expand. A natural flow, a natural mystic.
This year has started with a dream of an end, a death, my death. It has pointed at ancient Tibetan anthropology and legend. Of mild interest yes. Of real current world applicability to me, probably not. I do not move in circles where anything might be propagated. It is like a hint from an otherworld. It is very unlikely that Macron and the Dalai Lama have been discussing my future. Life on the compound will continue much as is. No biggie…
The surgeon was satisfied with his handiwork and I am due a follow up appointment with a different surgeon in March to discuss the cut and splice of my other leg. I have some ongoing physiotherapy. Aside from that currently the number density of medical appointments has fallen to a low. A bit of relative peace and quiet looks on the cards.
We have started the DIY tasks around the house and I have an exhortation to walk to help improve the use of my “new” bionic hip.
Maybe today I’ll try to use the sit on mower. This was prohibitively painful before the operation. If that works then we can save on the gardening fees…
The dreaming rate seems to have fallen from one every three days…to much a more sparse occurrence.
During the night I had a question:
“Is dreaming unidirectional? If I dream of someone do they dream of me?”
If you look on the internet you can find stoner questions. They ask things like:
“What do teeth taste like? Do everyone’s teeth taste differently?”
“If you have a Ph.D., does every meeting you go to become a doctor’s appointment?”
Far out man…
All that highfalutin stuff looks to be a simple curiosity to have a brief gander at and then move on…