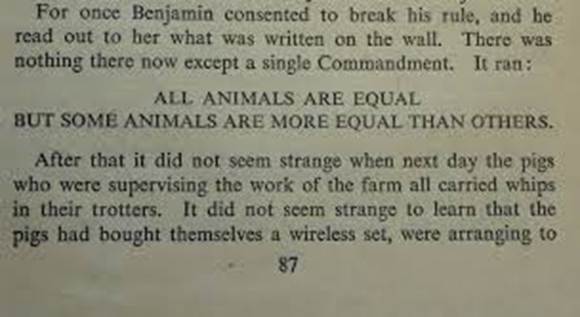
The world is pretty fucked up right now. When the butcher of Khan Yunis is nominating B2- “Obliteration”- Boi Trump for a Nobel Peace Prize things are more than a little topsy-turvy. This is perhaps a new(ish) if twisted reality for our times. If you remember Franco, Mussolini at al., the unpleasant people, once formed a bad-boys club before and that turned out well…
The world is heading into a very nasty phase. Brutality is holding dominion over compassion and humanity. Rife me-first separatism is being propagated, decency {and common sense} is subdued by the practice of domination, coercion and forced submission. The disproportionate exercise of power is once more in flow. Waving cocks is once again sadly de rigueur.
It is along way from any idyllic Kansas of ere.
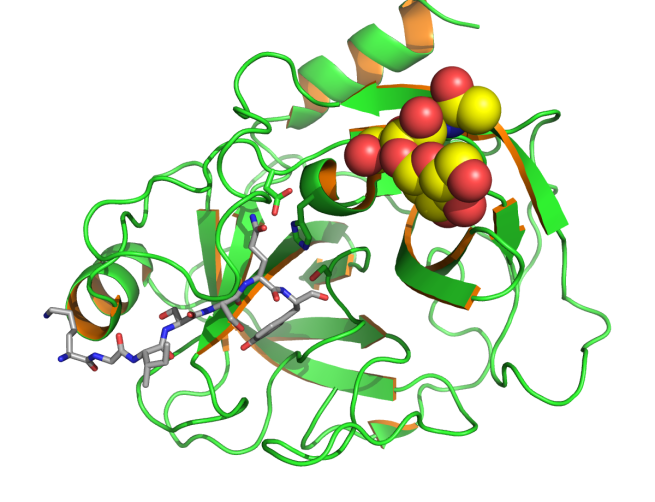
Today I get to find out if I have a heart amid all the high iron rust in my arteries and veins. They will probably plug me into the mains and look for traces of Fe2O3 in the pre-operative electrocardiogram. They may look for signs of a still pulsing muscle with an ultrasound device.
–

–
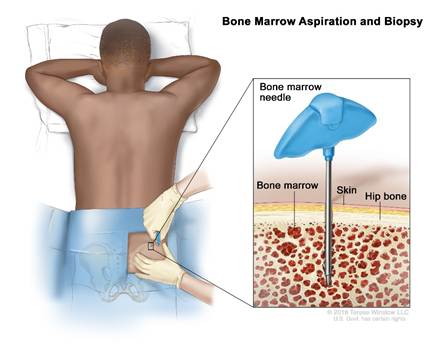
By the 18th of July I will have had 13 medical appointments in a little under three weeks. I will have given blood, had a CT and separate radionuclide scan {bonus CT also included}, a colonoscopy and test for sleep apnoea. I will have seen GP, implant dentist and consultant orthopaedic surgeons, a cardiologist, an osteopath, a rheumatologist and a lung specialist. That is a fair clustering of appointments. My dance card has been and is still full. In August I get to see a urologist for an update on my high prostate specific antigen levels. The next line of attack after the high res MRI I already have had is a prostate biopsy. Yippee!!! That will be fun. You can see from the look on my face above when they try to put a finger on it.
And on the TV in the news we get to see a stage managed travesty as mentioned in the first paragraph…
Are we really in this parallel universe. How the hell did we as a humanity get to this low low place. How much lower must we sink?? When this sort of thing seems quasi-normal?
This stinks, it smells real bad…